


Treatments for Gender Dysphoria.
Are we getting it right?

I have posted about this on my blog with the research paper attached. You can access this here 👇
The authors are listed below.
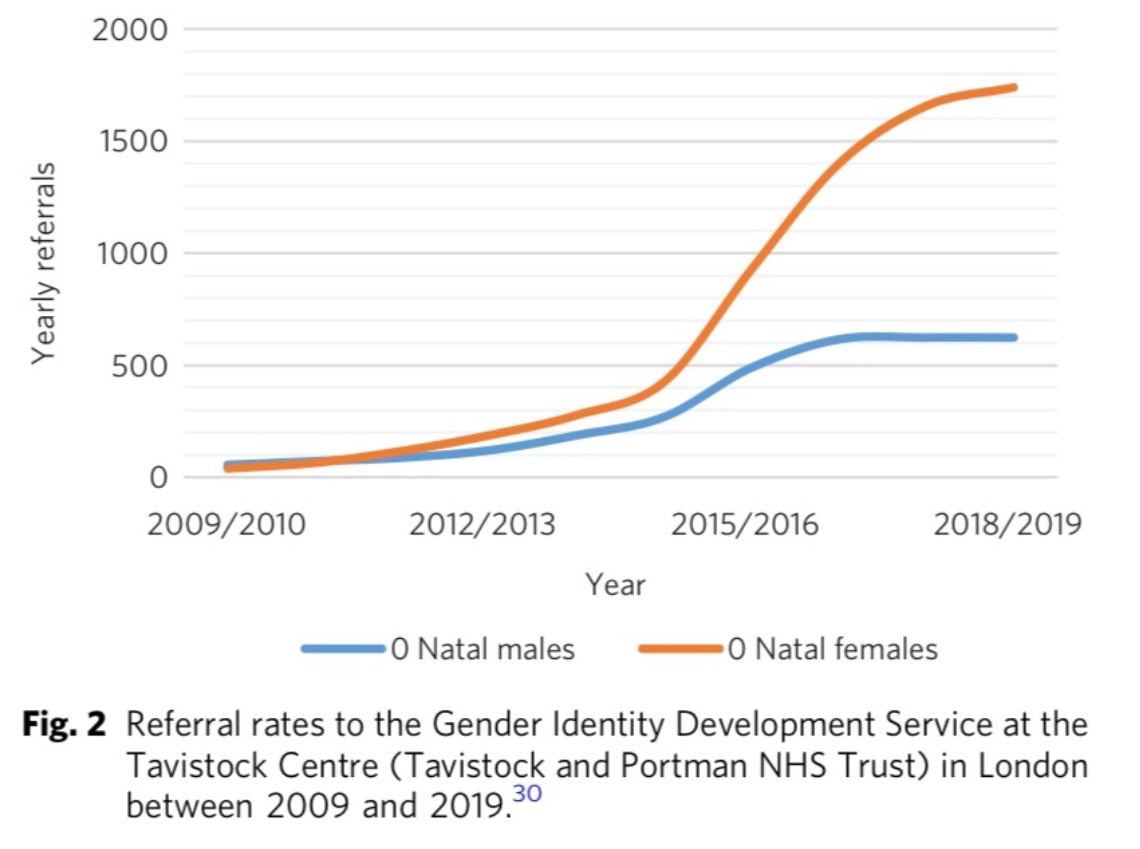
The authors are asking important questions about whether the treatment pathway for children and adolescents, who feel at odds with their biological sex, is the right one, It is imperative we interrogate this question in the light of growing numbers of referrals to Gender clinics, now a majority female. Historically this was a condition that affected males who made up the vast majority of referrals. Now referrals are up to 75% female which is a complete inversion of the sex ratios. The causes for this rise are hotly contested. However, it is an inescapable fact there has been a significant spike in referrals to Gender clinics. Below are the U.K figures since 2009. The increase is very pronounced for natal females. 👇
The authors look at the characteristics of new population and, in particular, they examine data relating to competing mental health issues. As you can see these include low mood, eating disorders, anxiety. Many are also on the autism spectrum.
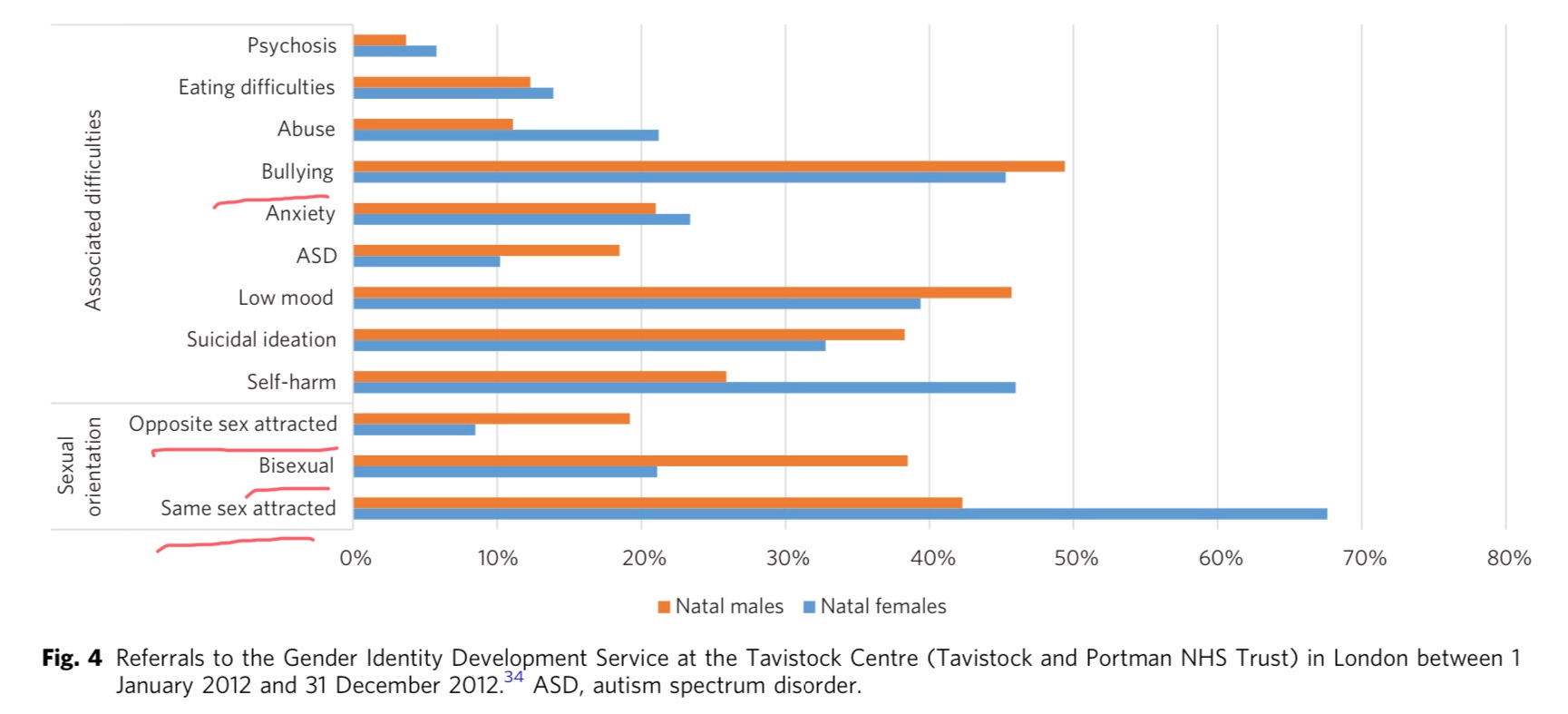
Moreover the referrals are tending not to be heterosexual. Nearly 70% of the females are same sex attracted and over 40% of the boys. This is even more pronounced if you look at those who identify as bisexual.
Another part of the referral population is kids in foster care. The authors note that there are 13% from the “looked after” sector based on Finnish Data: .
I have written about this phenomenon myself based on a paper from the Tavistock clinic. They also reported a higher than expected rate of foster + adopted children and adolescents in their patients. Combined these two groups comprised 13% of their patients. Foster kids made up over 4.9% of that total whilst the expected proportion, would have been in the region of 0.58%, based on that population. Interestingly they did not count children living with grandparents, as a distinct category, but included all children living with any biological family together. I would have liked to see disaggregated data on those not living with parents because separation from parents may also have produced attachment issues / unstable identity in these children. You can read my series on foster kids here :
Research on who is drawn to a transgender identity is vital to this understand this population. The reasons for this are contested because of the sway the “transgender child” has on those who are responsible for the treatment pathways. We should have paused irreversible treatments until we figured out was going on but we have actually become more aggressive with medical intervention; having started blocking puberty for children as young as ten.
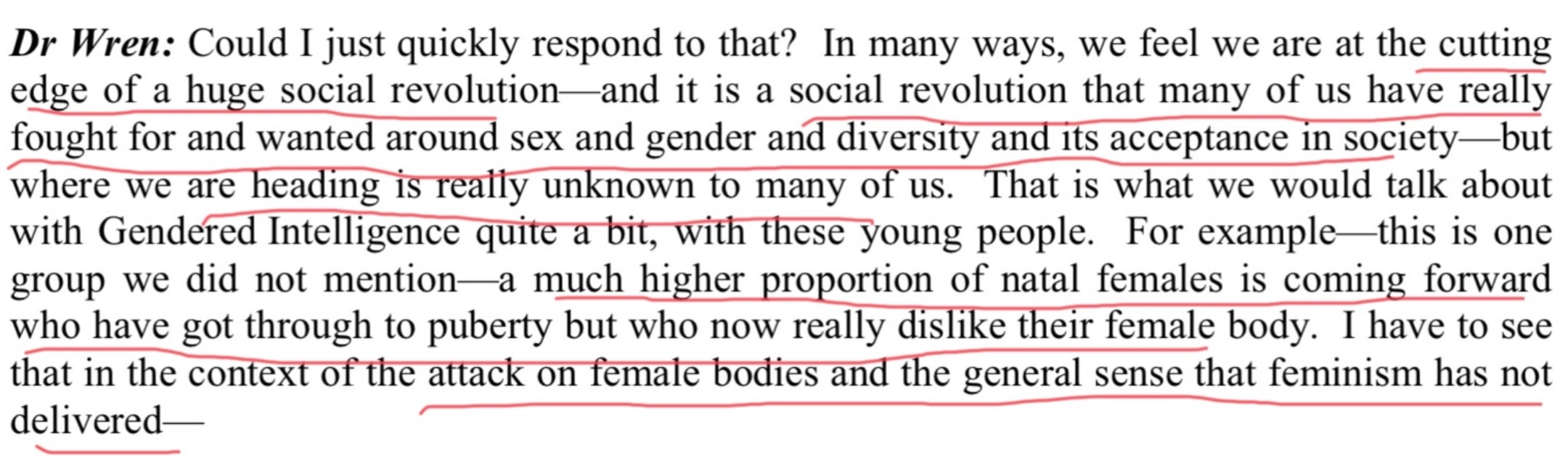
I recommend reading the entire paper but I will just leave you with this comment from Bernadette Wren from the Tavistock. This is from her appearance at a House of Commons Select Committee, so her statement was captured on Hansard. Has enthusiasm for a social revolution blinded these clinicians to the new form of self-harm they are enabling? How could you recognise a new form of female bodily hatred and still recommend these girls for double mastectomies?
There’s a tsunami of regret heading our way!
